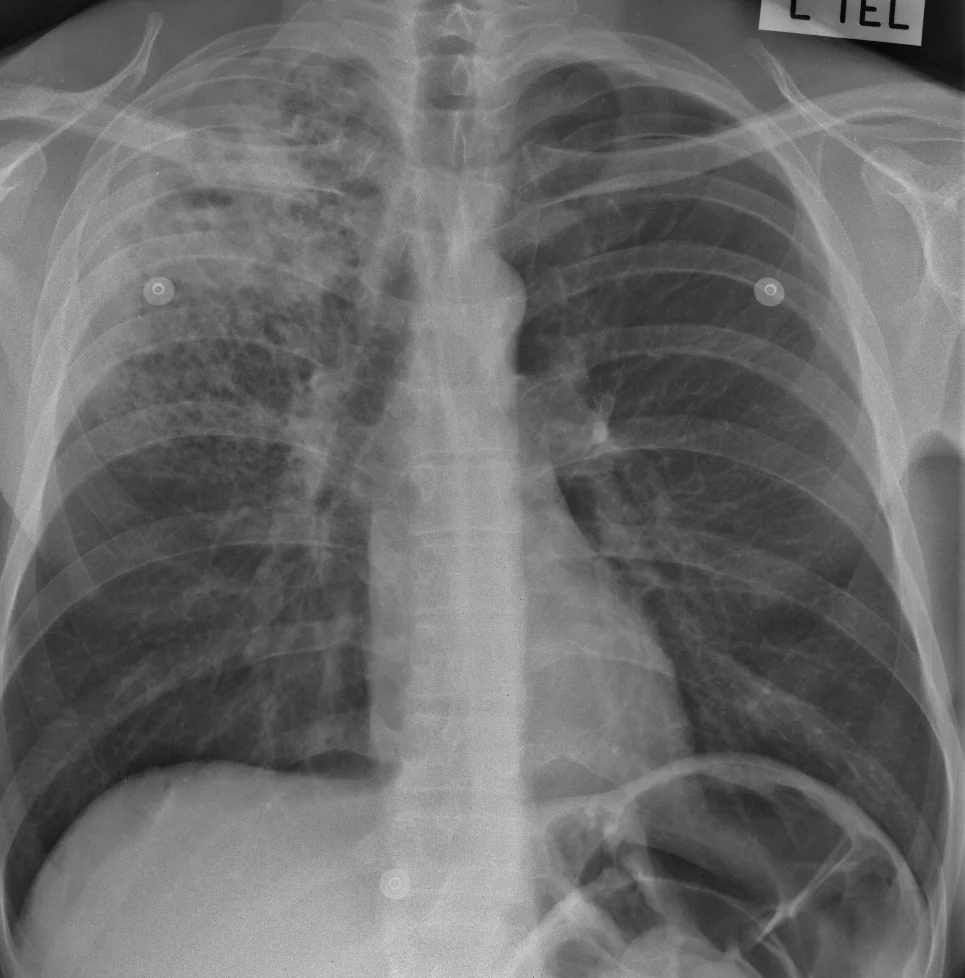
FIND: A huge number of tiny densities are scattered through both lungs. There is a circular dense line in the apex of the right lung. The right lung hilum is higher than normal. No other abnormality is seen.
Here is a magnified view of the right upper lobe:

IDENTIFY: A close-up shows that the lung looks as if it is made of thousands of little dots, or nodules, one or two mm in size. There are so many of them that we can't see the vessels any more. And the abnormality near the right lung apex has the appearance of a cavity with a smooth, thin wall. A high lung hilum usually means that it has been pulled up, either by a lobe which has lost volume or by scarring.
LABEL: There are thousands of tiny nodules scattered through both lungs, and there is a cavity at the right lung apex. The right lung hilum is pulled up but there is no sign of collapse (or atelectasis) of the right upper lobe. So it's likely that there is some fibrous scarring, which we cannot see because of the nodules.
MATCH: In a patient with this history the lung nodules are almost certainly due to miliary tuberculosis. The cavity and the presumed lung scarring also fit with tuberculosis. If the patient was not very ill, the nodules could be due to cancer metastases (although this is very uncommon), with underlying changes of old tuberculosis.
SUMMARISE: Miliary tuberculosis, with apical lung cavity likely due to tuberculosis as well. Right upper lobe scarring causing elevation of the right lung hilum.
Even though cancer is possible, TB would always have to be first on the list of diagnoses in an X-ray like this. Cancer would only be considered if TB could not be proven with sputum analysis and bood tests.
The right lung hilum is lower than the left hilum in 98% of normal people.
Note that this case is a little unusual, in that military TB is usually seen in primary infection, but this patient is an adult; he also has a lung cavity which is a sign of secondary tuberculosis. This reminds us that diseases don't always follow the rules, especially TB which is changing in the era of increased drug resistance and the effects of HIV/AIDS.